Nearly 800 million people are affected by mental health disorders around the world. Of these, depression and anxiety are the most common, affecting around 300 million each.
Awareness is an important part of finding help, which is where assessment tools are important.
Free DASS Test
The DASS is a widely-used psychometric test to check for the severity of symptoms of depression, anxiety and stress. Through 21 questions, the assessment expands each of these three into their individual symptoms, helping to explore your particular experience.
Organisations, practitioners and coaches can take the DASS assessment through Driven, which will provide a detailed report to help explore where are your people are at currently 📑
Got a Driven account?
Click the link below to take the DASS test now free:
No Driven account?
Create a free account here. Once you have an account, you can find the DASS test in the Explore menu under Mind & Mental Health.

A few unique things about Driven’s DASS report:
While the test and scoring methodology works the same, we flip the final scores around. Instead of getting a score for Depression, Anxiety and Stress, you’ll get a score for Enjoyment, Calmness & Relaxedness respectively. This is because our philosophy is to have something to work towards, rather than something to avoid.
In Driven’s DASS Report, you’ll get a much more detailed breakdown of your scores across the three main factors and also 16 subfactors. This helps you be more informed about your current experience and potentially what to focus on, particularly if working with a therapist.
Why provide a depression & anxiety test online for free?
The test itself is not a diagnosis of any disorder, but test results helps with self-education and seeking help.
For practitioners, read on to learn more about the DASS, how it works and how we’ve incorporated it into Driven to help connect these concepts with resilience.
DASS 21: PRACTITIONER GUIDE & MANUAL
DASS Manual
Below follows more detailed instructions on how the DASS works and related research.
As a practitioner, you can download our full guide to the DASS as implemented in Driven here for free.

Note that this isn’t a replacement for the manual provided by the original developers, which can be found here.
1. Introduction to the DASS Manual
The Depression, Anxiety, and Stress scale (DASS) has been widely used in both clinical and research contexts, both as a means of quantifying and differentiating each of these affective states.
This manual has been written to give resilience coaches a stronger theoretical and conceptual understanding of the DASS for usage within the Driven Resilience App and elsewhere.
Chapter 2 of this manual will provide a brief introduction and background to the DASS, some research justification on its effectiveness as well as outline some of its limitations.
Chapter 3 then delves into the structure of the DASS as well as its shorter variant, the DASS-21. A full breakdown of its items, the factors that the items assess and how it loads onto each scale is given.
Chapter 4 then provides practical guidelines around the application of the DASS.
Chapter 5 proceeds into the scoring and processing of the DASS, including automatic scoring provided by the Driven Resilience App.
Chapter 6 provides a breakdown of the results obtained from the DASS assessments. It also provides some suggestions as to how the resilience coach can help the participant dig deeper into the results given.
Chapter 7 delves into some of the specific psychometric properties of the DASS, particularly within the contexts that are relevant to its application through the Driven Resilience App.
Chapter 8 provides a brief overview of the construction of the DASS, including its intent and the method of its construction.
Finally, Chapter 9 provides a reading list for further reference.
2. Principle and Purpose of the DASS
Introduction
Feelings of depression, anxiety and stress can occur in anyone. These feelings can come and go for a variety of different reasons, and while some level of these may be considered natural or ‘normal’, it is when they reach a level where they interfere with our ability to live productive and meaningful lives that we need to consider intervention.
Naturally, our ideal is for this level of severity to be avoided through robust resilience capacity development which provides protection through a preventative approach. However, there are times when these symptoms still appear, and this is where an assessment tool is valuable.
What is the DASS?
The Depression, Anxiety and Stress Scale (DASS, or DASS scale) is a psychometric designed to rate the symptom severity across each of these factors. On this, the DASS offers a few unique pieces of information.
It allows both the participant and the coach to understand the scope of the participant’s emotional distress
It allows them to compare their own results with benchmark scores
It allows scientifically validated interventions to be applied to the individual and measured for improvement
Furthermore, the DASS is a unique scale because it distinguishes depression, anxiety and stress in a single validated scale. This enables us to better observe the close relationship between these three factors, and the phenomenon that each can cause the other. However, each factor has also been found to have different symptoms as well as different causes. This will be explored in more detail in the following section.
Theoretical Background
The Depression, Anxiety and Stress Scale was developed by Lovibond and Lovibond.1 It is one of many different measures that has been designed to measure the emotional state of its participants. The DASS provides not only an overall score which reflects an individual’s emotional state, but also the component scores of which one’s emotional state is comprised.
It is important to clearly define these different components here. Prior to Clark and Watson,2 the difference between depression and anxiety was strongly debated. They proposed the tripartite model of depression and anxiety, which suggested that the two displayed unique symptomology. Here, anxiety is characterised by heightened autonomic arousal. The autonomic nervous system is commonly known as the primary mechanism controlling the fight-or-flight response, and regulates bodily functions such as heart rate, digestion, respiratory rate, and sexual arousal. In the Anxiety Scale, the DASS then assesses whether the participant exhibits increased autonomic symptomology.
Alternatively, depression is characterised by a lack of positive affect. That is, individuals who are feeling depressed are those who are unable to feel pleasure in normally pleasurable activities. In the Depression scale, the DASS examines this lack of positive affect, as proposed by Clark and Watson,3 but also measures other features such as hopelessness and devaluation of life. This document will further expand on these in Chapter 3.
The way the word ‘Stress’ is used by Clark and Watson’s4 tripartite model of depression and anxiety is a little different from the way it is used in the DASS (outlined in Chapter 8). They also both use this term in a narrower sense than is commonly understood. Stress, within the DASS is characterised by the presence of negative affect.
Negative affectivity is the experience of negative emotions, including that of disgust, anger, guilt and fear.
Behaviourally, it is characterised by nervous tension, difficulty relaxing and irritability. The DASS then examines the presence of these symptoms in the Stress scale.
Characteristics of High Scorers
Individuals that score high for each factor (therefore showing more symptoms of the relevant factor), tend to exhibit particular characteristics. These may also be noticeable through conversation and observation. A list of these are shown below.
Characteristics of high scorers on each DASS Scale5
Depression Scale
Self-disparaging
Dispirited, gloomy, blue
Convinced that life has no meaning or value
Pessimistic about the future
Unable to experience enjoyment or satisfaction
Unable to become interested or involved
Slow, lacking in initiative
Anxiety Scale
Apprehensive, panicky
Trembly, shaky
Aware of dryness of the mouth, breathing difficulties, pounding of the heart, sweatiness of the palms
Worried about performance and possible loss of control
Stress Scale
Over-aroused, tense
Unable to relax
Touchy, easily upset
Irritable
Easily Startled
Nervy, jumpy, fidgety
Intolerant of interruption or delay
Psychometric Validity
The psychometric properties of the DASS have been verified across numerous contexts. Simply put, a measure (like DASS) should accurately and dependably measure its respective factors. Statisticians and psychologists are examining the psychometric properties of a measure, when they try to quantify its accuracy and dependability. There are many aspects examined regarding the psychometric properties, though two that are of significant interest are internal consistency (as a means to measure reliability) and construct validity (as a means of measuring validity). The psychometric properties of any measure used to support clinical diagnoses should be verified within specific contexts before it can be used within that context with confidence.
It is helpful, then, to know that the DASS is a widely used measure, with its psychometric properties validated across a broad array of contexts.
For example, the psychometric properties of the DASS have been verified in both clinical and non-clinical contexts. That is, it has been shown to be an accurate and dependable measure in people who have both been diagnosed with various mental health problems, and people within the general, broader population. Alternatively, where the psychometric properties of the DASS have been verified for both general adult as well as older adult populations, it may not be so accurate when used in adolescent populations. Finally, it must be noted that the reliability and validity of the DASS administered online has also been verified.6
More information regarding the reliability and validity of the DASS will be examined in Chapter 7.
Studies on clinical and non-clinical samples
Psychometric Properties of the 42-Item and 21-Item Versions of the Depression Anxiety Stress Scales in Clinical Groups and a Community Sample7
The psychometric properties of both the original DASS (with 42 questions) and the shortened DASS-21 (with 21 questions) were examined. This was done across both non-clinical (n=49) and clinical samples. Clinical samples included those diagnosed with panic disorder (n=67), obsessive compulsive disorder (n=54), social phobia (n=74), specific phobia (n=17) and major depressive disorder (n=46).
The internal consistency and internal validity of both the DASS and DASS-21 were found to be within acceptable to excellent ranges, across all samples.
The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non-clinical sample.8
The psychometric properties of the DASS were evaluated across a broad, non-clinical sample (n= 1,771).
The measure was shown to have adequate validity and excellent reliability scores within this sample.
Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples9
The psychometric properties of the DASS was evaluated across two large clinical samples (n= 437 and n=241).
The measure was shown to have an excellent internal consistency and internal validity within this sample.
Studies on older adult and adolescent populations
Psychometric properties of the Depression Anxiety and Stress Scale-21 in older primary care patients.10
The psychometric properties of the DASS-21 were evaluated across a sample of older adults (n=222) seeking medical care.
The measure was shown to have an excellent internal consistency and good internal validity within this sample.
Properties of the DASS‐21 in an Australian Community Adolescent Population.11
The psychometric properties of the DASS-21 were evaluated across a sample of adolescents (age=12-18, n=2873).
The measure was shown to have good reliability when measuring general distress in the adolescents, although the scales lacked specificity across all age groups.
The short version of the Depression Anxiety Stress Scales (DASS-21): Factor structure in a young adolescent sample.12
Alternatively, this study shows that symptoms of depression and anxiety are similar in adults and adolescents, but the measure of stress seems different.
While the research above includes age groups from 12 years old, the authors set the age limit at 14 years old and upwards for the DASS.
Some Limitations of its Use
A state measure of distress
The DASS is a measure of state (and not trait) anxiety and depression. That is, the measure does not look at whether the individual tends to be more depressed or anxious compared to other people (i.e.: whether it is part of their personality trait). It only looks at whether the individual has recently experienced symptoms of anxiety and depression (i.e.: what is their current emotional state). Although it may be more than likely that an individual with a depressive state might be experiencing a depressive emotional state, care needs to be used in understanding that those who score high in the depressive scale of the DASS might not be clinically depressed. Rather, there might be transient situational factors at play, such as a recent tragedy or personal setback that they are working through.
The DASS and diagnosis - Not a clinical diagnosis
Despite the DASS quantifying distress along the dimensions of depression, anxiety and stress, scoring high in any of these is not a clinical diagnosis. Clinical levels of distress should only ever be identified by a qualified professional, such as a psychologist. This measure, however, may be used by psychologists as one of a variety of tools used to ascertain such a diagnosis.
No indication for falsified results
An individual may falsify their answers for numerous reasons. They may feel the need to be perceived as better or worse than they are. They may have an inflated or deflated view of themselves. As with most psychometrics, the DASS has no means of checking whether results have been intentionally misstated.
3. The Structure of DASS
Driven uses both DASS as well as the shorter variant of the DASS scale, known as DASS-21. The DASS consists of 3 sets of 14 questions and the DASS-21 consists of 3 sets of 7 questions, with each set relating to one of the three scales of depression, anxiety and stress. Respondents are asked to base their responses as experienced over the last week. Responses are presented in a 4-point Likert scale, then scored between 0-3. Component scores are then compiled for each of the three scales, with a higher score indicating stronger symptomology. An overall score is also compiled, with a higher score indicating higher levels of generalised distress.
What is the DASS 21 questionnaire?
The DASS-21 has an obvious advantage over the DASS – as it consists of half the questions, it takes half the time to complete. The items of the DASS-21 have been selected from those within the DASS, and have been selected because of the following criteria:
Good factor loadings: those items found (through statistical analysis) to be most effective in measuring each factor have been chosen.
Even coverage of all scales across each scale
Ensuring item means of the DASS-21 is very similar to that of the DASS
Because of this, the DASS gives a little more reliability around specific symptoms of each affective state. Also, studies comparing the DASS and the DASS-21 show that the DASS gives slightly more reliable scores. You’ll notice as you read through the statements included in the full DASS, they are indeed highly similar statements – mainly expressed slightly differently and often reversed. Generally, the full DASS is more preferred in research, where the DASS-21 is often used for clinical purposes as the reduction in survey fatigue is preferred while reliability is maintained.
Note: For the following sections, questions marked with an asterisk (*) appear in the DASS-21 only.
Depression Test
Depression in a clinical sense has various associated symptoms related to it, including a persistent feeling of sadness, loss in interest and enjoyment in activities, and hopelessness. The DASS scale for depression examines seven key symptoms (subscales) of this, including dysphoria, hopelessness, devaluation, self-depreciation, lack of interest/involvement, anhedonia and inertia.
You may note that missing from these and the DSM-5 diagnostic criteria are symptoms of overeating or loss of appetite, as well as checking for suicidal ideation. While this omission may make the scale somewhat ‘friendlier’, especially when conducted online, it is important to be aware of this so they can be controlled for through further discussions with a client.
Dysphoria Subscale
Dysphoria is a general sense of unease, unhappiness, frustration, or dissatisfaction with life. Temporary moods of dysphoria can be quite normal, however if this becomes an ongoing (chronic) state which negatively impacts the ability of a person to enjoy life, then this is where we tend to see dysphoria being associated with mental health conditions. Common signs of dysphoria may also include apathy, sadness, and fatigue. To that extent, these questions explore the frequency of dysphoria experienced.
I felt downhearted and blue*
I felt sad and depressed
Hopelessness Subscale
Hopelessness can arise from feeling like there is no possibility for problems to be solved or improved, and is characterised by a sense of despair. Thoughts related to this might include feeling like things won’t get better, there’s no future, it’s too late, I will never be happy again, and so on. Having a sense of hope for the future is important for self-motivation, combining with a sense of optimism and passion to pursue activities and engage with life. Losing this sense of hope can be draining and leave little energy to work towards a better future. The questions here explore how often hopelessness was experienced.
I felt that I had nothing to look forward to*
I could see nothing in the future to be hopeful about
Devaluation Subscale
Lorem ipsum dolor sit amet,
Devaluation in this sense is a distortion of the value of something, seeing it instead as worthless, completely flawed, or not worth the effort. Here this is the opposite of idealization, such as seeing a person as ‘perfect’ and exaggerating their positive qualities. Idealization often leads to disappointment, however devaluation can lead to a lack of desire to engage and participate with something in the first place. In this case, the focus is on a big question: if life itself has been devalued, seeing it as something that’s not worth engaging in, and how often this feeling was experienced:
I felt that life was meaningless*
I felt that life wasn’t worthwhile
Self-Deprecation Subscale
In this context, self-deprecation is more closely related to the concept of self-worth. A strong sense of self-worth is a basic human need, providing a sense of confidence and internalised security that is characteristic of healthy self-esteem. In contrast, self-deprecating humour can be a charismatic quality displaying humility that is still backed up by a strong sense of self-worth and confidence. However, when the self is actually seen as being worthless, we move towards symptoms of depression as it may become disruptive in everyday life. The question explores the frequency of feelings of this:
I felt I wasn’t worth much as a person*
I felt I was pretty worthless
Lack of Interest/Involvement Subscale
Having an interest in various aspects of life is an important part of motivation. This can relate to engaging in hobbies, desiring to learn more about people, being curious about the world, interested in learning about oneself, setting goals & being interested in pursuing them, joining others with their goals, being excited about events coming up, and so on. For all these, interest and a desire to be involved is an important part of motivation. While we may often not feel interest in certain things, if we lose the ability to become interested or excited about anything, then it can become dysfunctional and exploration can be helpful. Here the questions explore frequency of a lack of interest & involvement:
I was unable to become enthusiastic about anything*
I felt that I had lost interest in just about everything
Anhedonia Subscale
Doing enjoyable things is one of the very basic and primal human needs. When we lose the ability to enjoy things that we used to enjoy, that is when we experience ‘anhedonia’. It’s not necessary for us to enjoy everything that we do. There can be many things that are simply not enjoyable to us, and that is quite natural. However, ideally we should still be able to enjoy certain things, such as a favourite TV show or music, talking to friends, reading a book, playing sports, and so on. It’s a common symptom of depression that we start to lose the enjoyment we used to feel with these activities, resulting in a decreased desire to engage with them again in the future. Here we explore the frequency of this experience:
I couldn’t seem to experience any positive feeling at all*
I couldn’t seem to get any enjoyment out of the things I did
Inertia Subscale
In life we can get into a groove where we have healthy habits that we stick to, such as showering in the morning, brushing teeth, getting breakfast, keeping rooms clean, going to work/school on time, and generally getting things done & staying on top of life. While these are often relatively small tasks, it sometimes happens that we just struggle to muster up the energy to do all these. This is where a common symptom of depression is not looking after oneself anymore, letting personal hygiene slip, and simply lacking the energy (or inertia) to keep doing all the daily things we need to. This can significantly affect the desire to take on bigger tasks and goals. When getting out of bed becomes a frequent struggle, then it’s worth investigating. These questions explore the frequency of this experience:
I found it difficult to work up the initiative to do things*
I just couldn’t seem to get going
Anxiety Test
There are various anxiety disorders, including phobias, panic disorder, post-traumatic stress disorder, obsessive compulsive disorder, social anxiety, and generalized anxiety disorder. These can take time to distinguish and have various different symptoms (subscales) related to them. This is a good example of why tests like DASS don’t provide a diagnosis, since the actual distinction between specific disorders generally take the care of a professional to properly diagnose.
Here, the DASS anxiety scale examines four different factors: autonomic arousal, skeletal musculature effects, situational anxiety and the subjective experience of anxious affects.
Autonomic Arousal Subscale
These questions all relate to the direct physiological symptoms of heightened autonomic arousal. This is primarily related to activation of the fight-or-flight systems controlled by the limbic brain, including the amygdala, the hypothalamic-pituitary-adrenal (HPA) axis, and the bed nucleus of the stria terminalis (BNST). The BNST maintains more consistent activation and thus may relate more to generalized anxiety, while amygdala activation tends to be fast and is more related to panic disorders and phobia.
Activation of the limbic brain increases certain hormones which result in noticeable physical effects. While occasional activation of this system is natural, when this activation becomes chronic and inappropriate (for example being afraid of something that’s benign), then it veers toward an anxiety disorder that can be improved through treatment.
I was aware of the action of my heart in the absence of physical exertion (e.g. sense of heart rate increase, heart missing a beat)*
I was aware of dryness of my mouth*
I experienced breathing difficulty (e.g. excessively rapid breathing, breathlessness in the absence of physical exertion)*
I perspired noticeably (e.g. hands sweaty) in the absence of high temperatures or physical exertion
I had difficulty in swallowing
Skeletal Musculature Effects Subscale
Increased activation of the limbic brain – in particular the HPA axis – increases adrenaline release and sympathetic nervous system activation. While many of the symptoms of this activation are not related to skeletal muscles, one skeletal symptom is shakiness which is often most easily observed in the hand. Occasionally experiencing this may be totally normal, however, ongoing occurrence of this may be symptomatic of an anxiety disorder, which is what this question screens for:
I experienced trembling (e.g. in the hands)*
I had a feeling of shakiness (e.g. legs going to give way)
Subjective Experience of Anxious Affect Subscale
While there are various physical symptoms related to anxiety, these are also accompanied by subjective experiences, such as feeling scared, panicked, terrified, and so on. Often these feelings are experienced without reasonable grounds to base them on. After all, there are times when panic and terror are entirely appropriate responses. However, when these appear with relative frequency at times when they are not helpful, then we are seeing symptoms of an anxiety disorder. These questions investigate the frequency of this experience:
I felt I was close to panic*
I felt scared without any good reason*
I had a feeling of faintness
I felt terrified
Situational Anxiety Subscale
Some anxiety disorders are related to a specific situation or experience. This may be a social situation (social anxiety disorder), going into an elevator (phobia), or something to that effect. Screening for various different situations would make for a cumbersome assessment, so the approach here is to rather screen for whether there were specific situations that resulted in excessive worry as a general occurrence. If this was indeed the case, then this can be further explored to examine the type of anxiety it might be related to so effective treatment can follow.
I was worried about situations in which I might panic and make a fool of myself*
I found myself in situations which made me so anxious I was most relieved when they ended
I feared that I would be “thrown” by some trivial but unfamiliar task
Stress Test
Stress is often a feeling of being under pressure. Exacerbating factors can be a time limit, major consequences connected to completion, and uncertainty. Here we may find acute stress, which could be related to a specific event coming up such as a work deadline, important exam or test, or public speaking event. We may also find chronic stress, which is ongoing and may be related to such situations as ongoing health problems or pain, caring for someone with high needs, dealing with ongoing harassment or bullying, financial stress, relationship issues, and so on.
Some degree of stress may be productive in that it can be experienced as motivating through pressure that is manageable within one’s cognitive and practical resources. However, chronic stress can result in overwhelm and burnout, causing a significant disturbance in the ability to manage everyday pressures and maintain personal relationships. Stress management techniques can be employed to help manage this condition.
The stress scale examines the presence of five symptoms (subscales), including: difficulty relaxing, nervousness, being easily upset/agitated, irritability/over-reactivity, and impatience.
Difficulty Relaxing Subscale
High stress situations may still be manageable if an ability is maintained to temporarily disconnect from the experience of stress and relax. A healthy state may be the ability to distance from stress so that even in periods of high stress, it’s not necessarily the case that the feeling of stress is consistent. An example may be the ability to ‘leave work at work’, being able in a sense to ‘forget’ about work issues on leaving work, and thereby maintaining an ability to be relaxed and recharge effectively at home and away from work. Conversely, when stress is constant or felt to such a degree that it becomes pervasive and influences every other aspect of life, then it may become dysfunctional. These questions screen for the extent of this occurrence:
I found it hard to wind down*
I found it difficult to relax*
I found it hard to calm down after something upset me
Nervousness Subscale
Similar to anxiety, stress can also activate the limbic brain and thereby the sympathetic nervous system. As adrenaline and cortisol increases, a feeling of nervous energy is experienced. This energy can again be useful in driving an individual to take action and work on the situation causing stress, however chronic activation of this can lead to feeling overwhelmed and eventually burnout may set in. These questions check for this experience of nervous energy and the frequency of this:
I felt that I was using a lot of nervous energy*
I was in a state of nervous tension
Easily Upset/Agitated Subscale
Being under a lot of pressure can result in someone being ‘tightly wound’, meaning they can easily become upset, angry, or agitated by small things. This can result in a disproportionate reaction to these small things such as not being able to find a matching pair of socks, a small stain on the carpets, or unwashed dishes in the kitchen. In the normal course of life, these are easily managed. But when under high stress, these can be the last straw that sets a person off. These questions screen for the frequency of these occurrences:
I found myself getting agitated*
I found myself getting upset rather easily
I found myself getting upset by quite trivial things
Irritability/Over-Reactivity Subscale
This symptom overlaps with being easily upset/agitated. Normally we may be able to handle unexpected events fairly well, such as a car breaking down, a financial emergency, an illness, and so on. But when under high stress, these situations can feel unmanageable, and sometimes even catastrophic, leading to an over-reaction that may not be helpful to resolve the situation. When this is noticed, bringing stress back to a manageable level can help to restore more constructive reactions to unexpected situations. These questions explore the frequency of this experience:
I tended to over-react to situations*
I felt that I was rather touchy*
I found that I was very irritable
Impatience Subscale
A stressful situation can cause an extreme form of prioritization, where anything that is not working directly towards the resolution of the source of stress is seen as simply being in the way. This can result in feelings of intolerance and impatience with anything that is preventing an individual from working on a specific task. These feelings may also crop up with any delay, such as unexpectedly slow traffic, people walking slowly, waiting for an elevator, too many emails and messages being received, and so on. These questions check for the experienced frequency of this type of impatience:
I was intolerant of anything that kept me from getting on with what I was doing*
I found myself getting impatient when I was delayed in any way (e.g. lifts, traffic lights, being kept waiting)
I found it difficult to tolerate interruptions to what I was doing
Generalised Distress Score
By combining the scores of the depression, anxiety and stress scales, a Generalised Distress Score can be produced. Currently, there is mixed support for the use of the Generalised Distress Score. There is disagreement as to what this score reflects, but the authors of the DASS argues that it is both possible and sensible to create and compare this score.13 Under their conception, as the scales of depression, anxiety and stress are independent factors of a generalised sense of distress, this score gives an overall indication of the scope of affective disorder experienced by the participant.
Resilience as a Mediator of Depression, Anxiety & Stress
While on the topic of depression, anxiety and stress, it’s useful to consider the interaction of resilience on these.
Resilience is well-understood as a mediator of all three, providing both relief as a treatment, while also acting in a protective capacity to avoid these in the first place.
Through the inclusion of DASS into the Driven platform, we hope to gain a better understanding of the interaction between resilience and depression, anxiety and stress. To this extent, let’s review a few indicators that illustrate the mediating effect of resilience.
How Resilience Mitigates Depression
There is a wealth of research on the positive effects of resilience techniques on depression. Here is a quick summary of some observations in the research:
Resilience helps regulate loneliness, which is a strong and rising risk factor for depression. Loneliness predicts how severe late-life depression can be14
Resilience strategies improve HPA axis regulation,15 which contributes to regulating depression
Resilience scores are useful to predict development of depression in the short term (under a year)16
Interventions at an individual, family, and community level can strongly impact the chance of developing depression. One study found that resilience interventions helped young refugees engage better in prosocial behaviour, which is a protective factor against depression17
In late-life depression resilience strategies can both prevent depression, “promote well-being even in the absence of current psychopathy” and be applied as a treatment to those with depression.18 Thus the authors advocate for widespread application regardless of whether or not someone is at obvious risk of depression
How Resilience Mitigates Anxiety
Anxiety is one of the most common mental disorders in the world.19 Therefore any mediating assistance from resilience is a strong encouragement as helpful training to undergo.
Higher resilience capacity combined with Generalized Anxiety Disorder (GAD) significantly improves response to adversity20
Higher resilience in children predicts better management of risks and helps them avoid adverse outcomes over time21
Mental resilience mediates the interaction between adverse childhood experiences and future emotional dysregulation. The higher the resilience, the lower the emotional dysregulation22
Resilience helps regulate the amygdala23
Depressed patients having both high resilience and low trait anxiety were about ten times more likely to achieve treatment response than those having either low resilience or high trait anxiety24
How Resilience Mitigates Stress
Resilience is well-known to help mediate the effects and perception of stress.
A person may inherit heighted reactivity to stress through their genes. However, the interaction between these genes and the person’s environment may be moderated through resilience strategies to reduce the stress response25
Resilience interventions in periods of stress help develop coping strategies and contribute to protective factors26
Resilience interventions result in higher problem solving and lower problem-avoidant behaviour; higher positive affect and self esteem27
Resilience interventions help lower signs of stress, like negative affect and depressive symptoms28
Resilience may help moderate several neurobiological factors that influence stress,29 such as:
Oxytocin
Prolactin
Dehydroepiandrosterone (DHEA)
Corticotropin-releasing hormone (CRH) effects on CRH-2 receptors
Neuropeptide Y
Galanin
Brain-derived neurotrophic factor (BDNF)
GABA-benzodiazepine receptors
Serotonin effects on the 5-HT1A receptors
Testosterone
-
Resilience may also mediate neural stress mechanisms,30 such as:
Regulation of reward
Social emotions
Non-social emotions
Motivations
Fear conditioning
-
Resilience counteracts direct negative impacts from stress31
4. Administering the DASS
Protocols have been established by the original authors of the DASS to maintain consistency of the results. It is important to follow the guidelines given below, as the standardisation of methodology will ensure the best results in data collection.
Who can participate in the DASS
Studies have confirmed the effectiveness of the DASS for adults and older adults in both clinical and non-clinical populations. However, it’s use with children and adolescents are not yet well supported. In adult populations, the use of the DASS has been shown to be effective across a large cross-section of racial and cultural backgrounds, genders and nationalities.
Who can apply the DASS
The DASS has been designed to be used as a self-administered measurement. That is, the instructions provided by the measure are generally enough to allow the DASS to be completed by a participant with no additional intervention. This makes the DASS effective to be delivered in an online self-serve format, however with the caveat this the result is not a diagnosis. Instead, it may provide a prompt for an individual to seek professional help and pursue psychoeducation.
Should the DASS be offered to individuals via the Driven Resilience App under the direction of a coach, it is important that the presence of the coach doesn’t influence the results. This can be done by following the guidelines below.
Providing instructions for the DASS
While the participants are completing the DASS it is important to not interact with them as this may influence their answers. If the participants have any questions while completing the DASS, it is best to encourage participants to try their best to answer the questions as they understand them. This is done to maintain consistency across the information presented to each participant. However, this shouldn’t often occur as the DASS should be presented with enough instructions for the participant to complete the measure without much trouble, and the items themselves are generally easily understood.
It may be deemed appropriate to verbally communicate instructions for completing the DASS with participants before they start the measure. Again, try to keep to only communicating information as provided in the measure.
Environment around application
Should you have many people concurrently completing the measure on their individual devices, it is important that there is no interaction between those individuals while they are doing so. They are free to share what they like after the completion of the task, but while participating they should not discuss meanings of questions, share or compare answers, or interact in any other way. They should also be discouraged from doing online searches, checking their messages or being distracted by anything else while they complete this task. Similarly, if the participant is completing the task without supervision, it is best to ensure that the individual is not interacting with other people, to focus on completing the task without distraction.
Who can interpret the results
When doing each of the scales or the full DASS through the Driven Resilience App, it will provide an output of not only the results, but also a brief interpretation of the results for each participant.
Of course, it is important to understand that the DASS does not serve as a diagnosis, but an indication of current emotional states.
It is suggested for resilience coaches to use the results as a tool towards developing an understanding of the participant’s emotional state.
5. Scoring and Processing the DASS
DASS-21 online test
The Driven Resilience App will automatically score the DASS-21, giving scores for the factors of depression, anxiety and stress. The results will then be presented in an easily understandable format right after completion. In this section, we will briefly cover how the DASS-21 is scored, to gain a full understanding of how the DASS-21 operates.
What is the difference between the DASS21 online and a paper test?
A frequent question is around any differences between delivering the DASS through an online or paper format. Both versions have been validated, allowing it to be administered through either format as needed. As the DASS 21 is generally the version used in practical applications, this is the version that’s used online in the Driven Resilience App.
The advantage of having it delivered online is that results are automatically calculated to provide quick and easy assessment. Driven therefore works as a DASS 21 calculator, automatically producing scores that speed up interpretation & action.
How does the DASS 21 scoring work?
Responses to each question are given on a four-point Likert scale. The responses range as follows:
0 Did not apply to me at all – NEVER
1 Applied to me to some degree, or some of the time – SOMETIMES
2 Applied to me to a considerable degree, or a good part of time – OFTEN
3 Applied to me very much, or most of the time – ALMOST ALWAYS
‘Never’ is scored the lowest (0) and ‘Almost always’ is scored the highest (3).
Each question relates directly to only one of the 3 scales of interest. As the DASS has 3 sets of 14 questions, and the DASS-21 has 3 sets of 7 questions, the highest score possible in any scale would be 42 and 21 respectively. Thus, while using the DASS, a score of 42 in the depression scale would indicate that the individual is reporting severe levels of depressive symptomology. Alternatively, while using the DASS-21, a score of 21 in the depression scale would indicate that the individual is reporting the same. For both, a score of 0 will indicate that the individual is not reporting any symptomology in that scale.
The scores from each of the scales can be totalled to form the generalised distress score. For the DASS, this results in a maximum score of 126. For the DASS-21, the maximum score is 63. Again, a high score indicates that the individual is reporting high levels of generalised distress, and a low score reflects low levels of distress.
If one had completed the full DASS, and another completed the DASS-21, it is still possible to compare these results. There is good coverage of all scales across each test – the DASS-21 is very similar to that of the full DASS. Simply double the scales and the overall score. This would only serve as a rough estimation, and should not be done for research purposes. Another way to even the scores out is to convert to a percentage, which is what Driven does.
The scored data will also be presented with an indication of severity. Note that these results do not reflect a clinical diagnosed level of severity, but a reflection of population means, as described in Chapter 6.
Within Driven, there is the option to take the DASS 21 as a full scale with all three scales, though there is also the option to do each test individually.
Driven’s scoring approach
The approach we take in Driven is to standardise all assessments to show a higher score as a ‘preferred’ score. Doing so helps to provide a friendlier scoring system that tends to align more with people’s expectations with tests in general. This means we generally phrase each factor in a constructive sense, helping put more of an optimistic, positive view on each factor that provides participants something to aim towards (a desirable state to achieve) – rather than simply something to avoid. For example, rather than aiming to avoid depression, the participant can view this as aiming to get more enjoyment out of life.
The result is the following three versions of these scales that can be done online through the platform:
‘Enjoyment’ - Driven’s Depression Test Online
The normal depression questions are posed and scored as per the DASS guidelines, though here the score is reversed to show an ‘enjoyment’ score instead, indicating the level to which a person is gaining enjoyment out of life as the opposite of depression.
‘Calmness’ - Driven’s Anxiety Test Online
Here the normal anxiety questions are posed and scored as per the DASS guidelines, though the score is reversed to show ‘calmness’ score instead. This allows the individual to aim for a higher score, indicating a level of calmness as the opposite of anxiety.
‘Relaxedness’ - Driven's Stress Test Online
As above, the normal stress questions are posed and scored as per the DASS guidelines, though here the score is reversed to produce a ‘relaxedness’ score, indicating a state that is the opposite of stress in this instance.
Increased options
Naturally, the questions and application of the scales remain the same, so the validity remains untouched. The only difference being the reversing of the scores in the end and the phrasing of the factor.
Being able to do these tests separately online opens up further options, such as only doing a quick online anxiety test, or just a stress test, or any appropriate combination of the three.
Privacy Policy
This data will be analysed and stored under the same policy as outlined in Driven’s Privacy Policy. The Privacy Policy can be accessed via the app, or through the following web address: https://hellodriven.com/privacy
DASS Score Sheet
While the DASS can be performed through Driven for free with an automated report generated to help with analysis, you can also download a scoring sheet for the DASS here for manual collection and calculation – http://www2.psy.unsw.edu.au/dass/down.htm
DASS 21 Scores & Score Sheet
With the shortened version, DASS 21 scoring is quite similar. Once again, the response form and score sheet can be found here for manual collection and calculation – http://www2.psy.unsw.edu.au/dass/down.htm
6. How to Interpret the DASS
The Driven Resilience App will automatically calculate and display results for each scale both as a numerical score and in a visual format, alongside a score and description of each related subscale. This will provide an initial reflection on the current state of the participant within the scales of depression, anxiety and stress. The following interpretation provides additional guidance on interpreting scores.
To establish a basic interpretation of the scale scores, the table below shows range scores alongside classifications of severity as developed by the DASS’ original authors.
What do DASS scores mean?
The classification of each scale is an indication of severity of the symptoms. Keep in mind that these scores (even at an ‘extremely severe’ level) are not a diagnosis of each measure. An actual diagnosis will need to be made by a professional separately. These scores merely inform of the severity of symptoms currently experienced.
Classifications of scores for DASS36
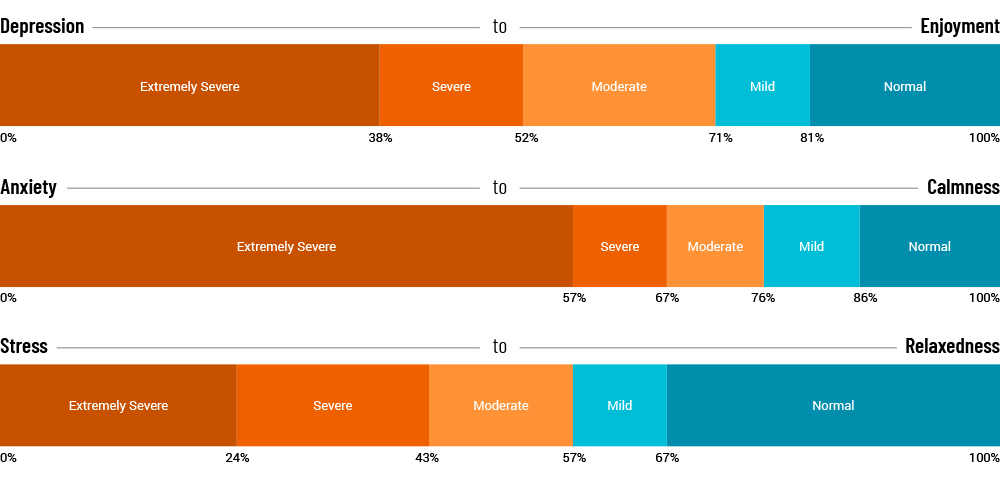
Depression
Normal: 0-19% (0-9)
Mild: >19-29% (10-13)
Moderate: >29-48% (14-20)
Severe: >48-62% (21-27)
Extremely Severe: >62% (28+)
Anxiety
Normal: 0-14% (0-7)
Mild: >14-24% (8-9)
Moderate: >24-33% (10-14)
Severe: >33-43% (15-19)
Extremely Severe: >43% (20+)
Stress
Normal: 0-33% (0-14)
Mild: >33-43% (15-18)
Moderate: >43-57% (19-25)
Severe: >57-76% (26-33)
Extremely Severe: >76% (34+)
Notice that the range within each description is different between each scale. These descriptions have been given based on the population means as found by Lovibond and Lovibond.37
As comparison for the DASS, they provided classifications on the basis of percentile scores, with those with 0-78% classified as ‘normal’ (that is, 78% of the population score at a ‘normal’ level), 78-87% as ‘mild’, 87-95% as ‘moderate’, 95-98% as ‘severe’, and 98-100% as ‘extremely severe’, based on the results of a non-clinical sample of adults.
Therefore, someone that scores in the Mild range still has more symptoms than the general population, even though the symptoms themselves are not severe.
Within Driven’s DASS report, a further explanation of the score and each subscale is provided to assist with understanding symptomology.
7. DASS 21 Reliability and Validity
Below are a few examples of validation conducted using the DASS. Note that there are many more research papers available with further information, so this does not present a complete list.
The DASS in research
Psychometric Properties of the 42-Item and 21-Item Versions of the Depression Anxiety Stress Scales in Clinical Groups and a Community Sample38
Both the DASS and DASS-21 were examined across both non-clinical (n=49) and clinical samples. Clinical samples included those diagnosed with panic disorder (n=67), obsessive compulsive disorder (n=54), social phobia (n=74), specific phobia (n=17) and major depressive disorder (n=46).
Internal consistency: Cronbach’s alpha for the Depression, Anxiety, and Stress scales were .97, .92 and .95 respectively. Cronbach’s alpha for DASS-21 scales was .94, .87, and .91.
Concurrent Validity: The DASS and the DASS-21 scales were compared against each other, as well as 3 other measures: the Beck Depression Inventory (BDI), the Beck Anxiety Inventory (BAI), and the State-Trait Anxiety Inventory, Trait version (STAI-T).
The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non-clinical sample.39
The DASS was evaluated across a general population of adults within the UK (n= 1,771).
Internal Consistency: Cronbach’s alpha for the Depression, Anxiety, and Stress scales where .947, .897 and .933 respectively. A Cronbach’s alpha for the total score was also tabulated, with a result of .966.
Concurrent Validity: The DASS was compared against the Hospital Anxiety and Depression Scale (HADS), the Personal Disturbance Scale (SAD) and the Positive and Negative Affect Schedule (PANAS).
Psychometric properties of internet-administered versions of Penn State Worry Questionnaire (PSWQ) and Depression, Anxiety, and Stress Scale (DASS)40
The DASS was evaluated in a sample of undergraduate students from the USA (n=1138). Here the DASS was applied via the internet.
Internal Consistency: Cronbach’s alpha for the Depression, Anxiety, and Stress scales where .95, .93 and .94 respectively.
Test-Retest & Concurrent Validity: Here, the DASS was compared with the Penn State Worry Questionnaire (PSWQ).
8. Construction of DASS
Developed by Lovibond and Lovibond41 between 1979-1990, the DASS was attempting to fulfil several key goals:
First, they sought to create a measure which examined the full range of core symptoms unique to anxiety and depression
Second, they sought to create a measurement which provided maximal discrimination between anxiety and depression
Third, they sought to create a measure which met high psychometric standards
In the following section, we will examine the background as to why each of these goals were established, and the processes undertaken meet these goals.
Goal 1: Core Symptoms of Anxiety and Depression
Depression and anxiety are understood to be quite distinct, however, a strong relationship between the two has long been observed.
There are many different theories as to how the two are related, as summarised by Clark and Watson.42 These include:
Being two points upon the same continuum
Alternative manifestations of a common underlying diathesis
Heterogeneous syndromes that are associated because of shared subtypes, featuring separate phenomena, which may develop into the other over time, and conceptually and empirically distinct phenomena
Clark and Watson43 found that although depression and anxiety share a non-specific component which causes general negative affectivity amongst other symptoms, the two can be distinguished by symptoms which are unique to each. Depression could be distinguished from anxiety by the lack of positive affect, where anxiety can be distinguished from depression through the presence of physiological hyperarousal (further explanation found in Chapter 2).
Knowing the symptoms which separated depression and anxiety, the DASS was developed to quantify each independently from each other, which leads to the second goal.
Goal 2: Maximal Discrimination
Lovibond and Lovibond44 listed the problems with existing methods used to measure anxiety and depression. They include:
Self-report anxiety and depression scales typically correlate between 0.40 and 0.70 across a wide range of patient and non-patient samples
Anxiety scales frequently correlate as highly with depression scales, and depression scales show equal lack of specificity
Clinicians’ ratings of anxiety and depression duplicate the relationships found with self-report scales
Only about half the patients diagnosed as having a depressive or an anxiety disorder exhibit relatively pure syndromes of one type or the other
As seen in the list above, not only were existing scales inefficient when discriminating between anxiety and depression, but clinicians had similar problems discriminating between the two. This then also affected the diagnosis that patients were given. This underscores the importance of obtaining a scale which provides for maximal discrimination between anxiety and depression.
Research and Development Methodology
The aim underlying the development of the DASS scales was to be guided by existing clinical conceptions of depression and anxiety, but ultimately determined by statistical analysis on empirical data.
To do this, items of the scales were developed by initially creating items based on clinical consensus. This was then refined empirically by using a confirmatory factor analytic technique with a multiple groups factor analysis (see Lovibond, Lovibond45). Items were added and deleted over the application of procedure of successive iterations, and was developed within general, non-clinical samples.
Development of the Stress Scale
It was during this time of research and development that the stress scale was also isolated in the DASS. Lovibond and Lovibond46 compiled a group of similar items from the research, items which did not help discriminate between anxiety and depression, into a single factor. This factor was called ‘stress’ as it had strong similarities to the symptoms of tension or stress, and included items such as ‘difficulty relaxing, nervous tension, irritability and agitation.’ Thus, where Clark and Watson47 saw stress as the generalised negative affect and other symptoms shared between depression and anxiety, stress within the DASS is conceived of as its own independent factor.
Goal 3: High Psychometric Standards
The emphasis put upon the development of the DASS to use empirical data contributed to its strong psychometric properties. Further research supports this, with some outlined in the previous chapter.
Conclusion
Overall, the DASS provides a reliable approach to assess depression, anxiety and stress, and provides insight into more specific symptomology that assists with treatment and intervention. Due to this we recommend this as an addition to coaching & clinical practice. To simplify application, Driven’s free DASS online test provides a detailed report that makes it easy to access this useful psychometric.
9. DASS Publications & References
Research used in this publication is cited below.
1. Lovibond, P.F. & Lovibond, S.H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33, 335-343.↩
2. Clark, L.A., & Watson, D. (1991). Tripartite Model of Anxiety and Depression: Psychometric Evidence and Taxonomic Implications. Journal of Abnormal Psychology, 100(3), 316-336.↩
3. Clark, L.A., & Watson, D. (1991). Tripartite Model of Anxiety and Depression: Psychometric Evidence and Taxonomic Implications. Journal of Abnormal Psychology, 100(3), 316-336.↩
4. Clark, L.A., & Watson, D. (1991). Tripartite Model of Anxiety and Depression: Psychometric Evidence and Taxonomic Implications. Journal of Abnormal Psychology, 100(3), 316-336.↩
5. http://www2.psy.unsw.edu.au/groups/dass/over.htm↩
6. Zlomke, K. (2009). Psychometric properties of internet administered versions of Penn State Worry Questionaire (PSWQ) and Depression, Anxiety, and Stress Scale (DASS). Computers in Human Behaviour, 25 (4), 841-843.↩
7. Antony, M.M., Bieling, P.J., Cox, B.J., Enns, M.W. & Swinson, R.P. (1998). Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales (DASS) in clinical groups and a community sample. Psychological Assessment, 10, 176-181.↩
8. Crawford, J.R. & Henry, J.D. (2003). The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non-clinical sample. British Journal of Clinical Psychology, 42, 111-131.↩
9. Brown, T.A., Korotitsch, W., Chorpita, B.F. & Barlow, D.H. (1997). Psychometric properties of the Depression Anxiety Stress Scales (DASS) in clinical samples. Behaviour Research and Therapy, 35, 79-89.↩
10. Gloster, A.T., Rhoades, H.M., Novy, D., Klotsche, J., Senior, A., Kunik, M., Wilson, N., & Stanley, M.A. (2008). Psychometric properties of the Depression Anxiety and Stress Scale – 21 in older primany care patients. Journal of Affective Disorders. 110(3) 248-259.↩
11. Shaw, T., Campbell, M.A., Runions, K.C., & Zubrick, S.R. (2017). Properties of the DASS-21 in an Australian Community Adolescent Population. Journal of Clinical Psychology. 73(7).↩
12. Szabó, M. (2010). The short version of the Depression Anxiety Stress Scales (DASS-21): Factor structure in a young adolescent sample. Journal of Adolescence, 33, 1-8.↩
13. http://www2.psy.unsw.edu.au/dass/DASSFAQ.htm#_26.__Is_the_total_DASS_score_a_usef↩
14. Holvast, F. et al. Loneliness is associated with poor prognosis in late-life depression: Longitudinal analysis of the Netherlands study of depression in older persons. J. Affect. Disord. 185, 1–7 (2015).↩
15. Gothe, N. P., Keswani, R. K. & McAuley, E. Yoga practice improves executive function by attenuating stress levels. Biol. Psychol. 121(Pt A), 109–116 (2016).↩
16. Wu, Y., Sang, Z. Q., Zhang, X. C., & Margraf, J. (2020). The Relationship between resilience and mental health in Chinese college students: A longitudinal cross-lagged analysis. Frontiers in Psychology, 11, 108.↩
17. Ziaian, Tahereh, Helena de Anstiss, Georgia Antoniou, Peter Baghurst, and Michael Sawyer. “Resilience and its association with depression, emotional and behavioural problems, and mental health service utilisation among refugee adolescents living in South Australia.” International Journal of Population Research 2012 (2012). ↩
18. Laird, K.T., Krause, B., Funes, C. et al. Psychobiological factors of resilience and depression in late life. Transl Psychiatry 9, 88 (2019).↩
19. Wittchen, H. U. (2002). Generalized anxiety disorder: prevalence, burden, and cost to society. Depression and anxiety, 16(4), 162-171.↩
20. Charney, D. S. (2004). Psychobiological mechanisms of resilience and vulnerability: implications for successful adaptation to extreme stress. American journal of Psychiatry, 161(2), 195-216.↩
21. Fergus, S., & Zimmerman, M.A. (2005). Adolescent resilience: A framework for understanding healthy development in the face of risk. Annual Review of Public Health, 26, 399–419↩
22. Poole, J. C., Dobson, K. S., & Pusch, D. (2017). Anxiety among adults with a history of childhood adversity: Psychological resilience moderates the indirect effect of emotion dysregulation. Journal of affective disorders, 217, 144-152.↩
23. Charney, D. S. (2004). Psychobiological mechanisms of resilience and vulnerability: implications for successful adaptation to extreme stress. American journal of Psychiatry, 161(2), 195-216.↩
24. Min, J. A., Lee, N. B., Lee, C. U., Lee, C., & Chae, J. H. (2012). Low trait anxiety, high resilience, and their interaction as possible predictors for treatment response in patients with depression. Journal of affective disorders, 137(1-3), 61-69.↩
25. Ellis, B. J., & Boyce, W. T. (2008). Biological sensitivity to context. Current directions in psychological science, 17(3), 183-187.↩
26. Steinhardt, M., & Dolbier, C. (2008). Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. Journal of American college health, 56(4), 445-453.↩
27. Steinhardt, M., & Dolbier, C. (2008). Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. Journal of American college health, 56(4), 445-453.↩
28. Steinhardt, M., & Dolbier, C. (2008). Evaluation of a resilience intervention to enhance coping strategies and protective factors and decrease symptomatology. Journal of American college health, 56(4), 445-453.↩
29. Davydov, D. M., Stewart, R., Ritchie, K., & Chaudieu, I. (2010). Resilience and mental health. Clinical psychology review, 30(5), 479-495.↩
30. A. Feder, E.J. Nestler, D.S. Charney Psychobiology and molecular genetics of resilience. Nature Reviews. Neuroscience, 10 (2009), pp. 446-457↩
31. Zimmerman, M. A., & Brenner, A. B. (2010). Resilience in adolescence: Overcoming neighborhood disadvantage. https://psycnet.apa.org/record/2010-10101-014↩
32. Masten, A. S., Best, K. M., & Garmezy, N. (1990). Resilience and development: Contributions from the study of children who overcome adversity. Development and psychopathology, 2(4), 425-444.↩
33. Anyan, F., & Hjemdal, O. (2016). Adolescent stress and symptoms of anxiety and depression: Resilience explains and differentiates the relationships. Journal of affective disorders, 203, 213-220.↩
34. Hoge, E. A., Austin, E. D., & Pollack, M. H. (2007). Resilience: research evidence and conceptual considerations for posttraumatic stress disorder. Depression and anxiety, 24(2), 139-152.↩
35. J.R. Davidson, V.M. Payne, K.M. Connor, E.B. Foa, B.O. Rothbaum, M.A. Hertzberg, R.H. Weisler, Trauma, resilience and saliostasis: effects of treatment in post-traumatic stress disorder, International Clinical Psychopharmacology, 20 (2005), pp. 43-48↩
36. https://www.psytoolkit.org/survey-library/depression-anxiety-stress-dass.html↩
37. Lovibond, P.F. & Lovibond, S.H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33, 335-343.↩
38. Antony, M.M., Bieling, P.J., Cox, B.J., Enns, M.W. & Swinson, R.P. (1998). Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales (DASS) in clinical groups and a community sample. Psychological Assessment, 10, 176-181.↩
39. Crawford, J.R. & Henry, J.D. (2003). The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non-clinical sample. British Journal of Clinical Psychology, 42, 111-131.↩
40. Zlomke, K. (2009). Psychometric properties of internet administered versions of Penn State Worry Questionaire (PSWQ) and Depression, Anxiety, and Stress Scale (DASS). Computers in Human Behaviour, 25 (4), 841-843.↩
41. Lovibond, P.F. & Lovibond, S.H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33, 335-343.↩
42. Clark, L.A., & Watson, D. (1991). Tripartite Model of Anxiety and Depression: Psychometric Evidence and Taxonomic Implications. Journal of Abnormal Psychology, 100(3), 316-336.↩
43. Clark, L.A., & Watson, D. (1991). Tripartite Model of Anxiety and Depression: Psychometric Evidence and Taxonomic Implications. Journal of Abnormal Psychology, 100(3), 316-336.↩
44. Lovibond, P.F. & Lovibond, S.H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33, 335-343.↩
45. Lovibond, P.F. & Lovibond, S.H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33, 335-343..↩
46. Lovibond, P.F. & Lovibond, S.H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33, 335-343.↩
47. Clark, L.A., & Watson, D. (1991). Tripartite Model of Anxiety and Depression: Psychometric Evidence and Taxonomic Implications. Journal of Abnormal Psychology, 100(3), 316-336.↩